Guest Author: Jack LeDonne MD, FACS, VA-BC
We are excited to welcome back Jack LeDonne, MD, FACS, VA-BC to the Eloquest Healthcare Blog! Dr. LeDonne hails from Brooklyn, NY. He graduated from Fordham University and St. George’s University, School of Medicine, in Grenada. Dr. LeDonne completed his surgical residency at the Wyckoff Heights Hospital, in Brooklyn, and fellowships at the Shock-Trauma Center and Harvard Medical School. He is presently the Medical Director at Chesapeake Vascular Access. Dr. LeDonne has ten clinical publications to his credit and is a strong believer in the power of video as an educational tool. He is a Fellow of the American College of Surgeons, Vascular Access Board Certified and a past president of the Association for Vascular Access. Dr. LeDonne was the recipient of the 2018 Suzanne Herbst Award for Excellence in Vascular Access.
In the following blog, Dr. LeDonne shares his top recommendations for: Modern Vascular Access related to Central Vascular Access Devices (CVADs). But first, in this brief video, he outlines the Life Cycle of Central Venous Catheters.
The Goal
The goal of Modern Vascular Access is to standardize practice at the highest level because we work on human beings. The major benefit of Standardization is that it eliminates unnecessary variation and unnecessary variation will hobble your outcomes.
Vascular Access Devices have a Life Cycle that consists of five phases:
- Assessment
- Pre-Insertion (the Insertion Bundle)
- Actual Insertion of the Device
- Care and Maintenance (C&M)
- Removal
We will use Pre-Insertion (Phase 2) as the model. The Insertion Bundle elements are uniformly standardized around the world. We would like to standardize the other phases of the Life Cycle just as the Insertion Bundle is standard.
The Assessment
The Assessment Phase (1) is vital, the goals in this phase are to determine what are appropriate and inappropriate indications for the CVAD and to evaluate the various Central Veins with Ultrasound for suitability of cannulation. There are guidelines, e.g., MAGIC, DAV-Expert and others to help standardize the Assessment Phase.
The national standard for insertion of a CVAD is the Insertion Bundle (Phase 2). However, the Insertion Bundle stops at an inconvenient spot, namely the actual insertion of the device. Once the patient is draped for the procedure, the Insertion Bundle is over. But there is much more in the Life Cycle, i.e., actual insertion and C&M, and these phases should be performed in standardized fashion at the highest level, as well.
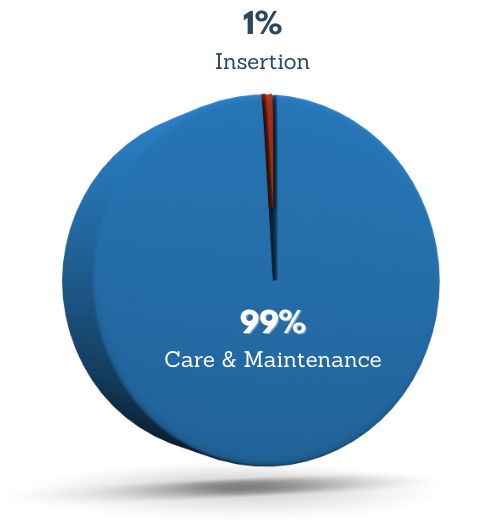
Regarding the Actual Insertion of the CVAD and the C&M (Phases 3 and 4), the Insertion accounts for 1% of the Life Cycle and C&M is 99%; therefore, the Insertion should be performed in a standardized fashion that enables optimal C&M. The relationship between the Insertion and C&M is rarely discussed but is vital to a successful outcome for a CVAD that is free of complications.
The Insertion
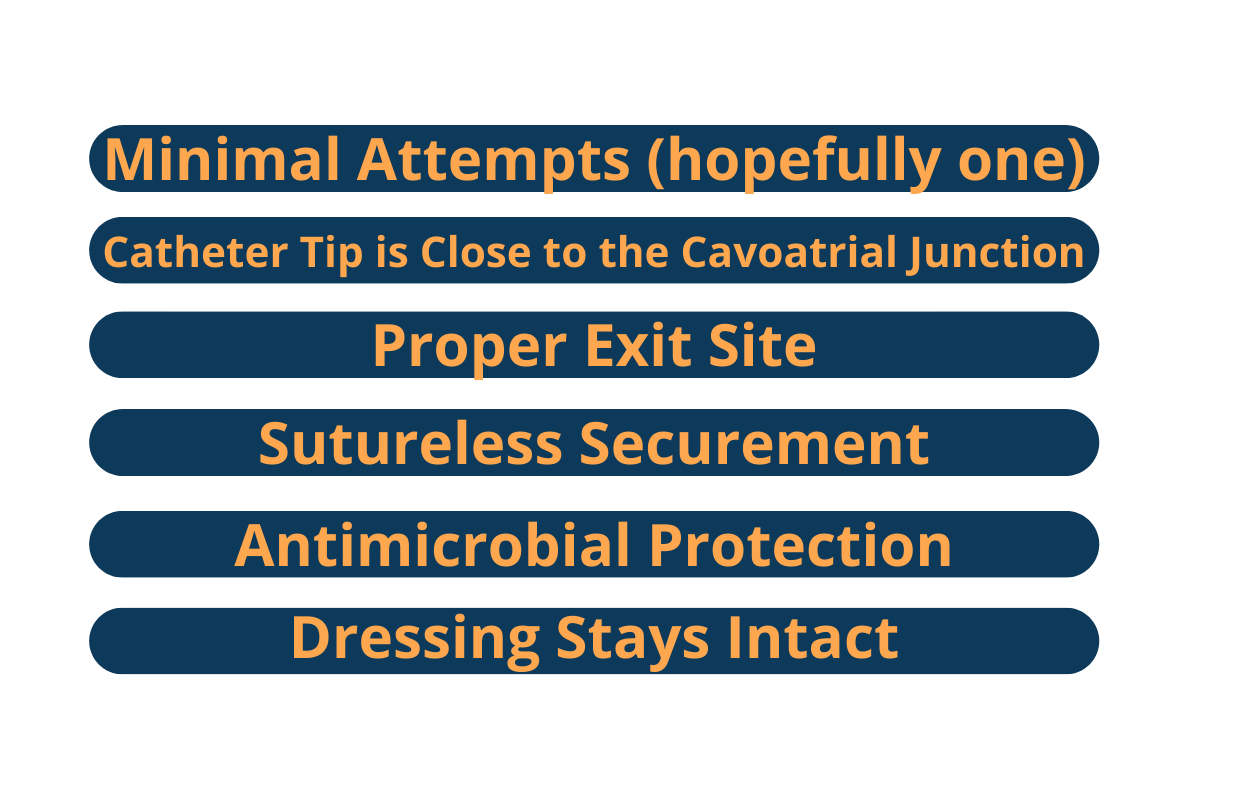
Listed here is what constitutes a proper standardized insertion! Just as the forearm is the preferred site for a peripheral IV cannula and the middle of the arm is preferred for midlines and Peripherally Inserted Central Catheters, there is an optimal exit site and dressing location for CVADs, i.e., the chest. The chest is a relatively flat surface that exhibits minimal motion compared to the neck. Motion is the enemy of an intact dressing. If it is not possible to achieve an exit site/dressing on the chest, then low cervical/supraclavicular is preferable to the middle or upper neck.
The Achievement
There are three methods to achieve a dressing on the chest, all of which employ ultrasound guidance. The first technique is to cannulate a vein on the chest. When using ultrasound, the name of the vein is the Axillary Vein. The second technique is to cannulate the Internal Jugular (or Brachiocephalic) Vein, low in the neck, and rotate the catheter downwards onto the chest. The catheter will not kink. The third method is to puncture the Internal Jugular (or Brachiocephalic) and tunnel the catheter subcutaneously to the chest. This is performed at the bedside, without fluoroscopy, and like the first two techniques employs ECG guidance for catheter tip location. Of special note, in the spirit of Standardizing practice at the highest level, we never puncture in the middle or upper neck, and we never direct the catheter upwards, toward the mandible or the ear. If the catheter is directed upwards, gravity will grab the tails and pull them towards the floor, disrupting the dressing.
The Proof
Timsit demonstrated that 67% of CVAD dressing changes were unscheduled and that disrupted dressings were a major factor related to Blood Stream Infections.¹ The goal for the dressing (99% of the CVAD Life Cycle) is for the dressing to be 100% intact for seven days. In contradistinction to the goal of seven days, Richardson studied four popular dressings and found that the best one stayed intact for 68 hours and the other three remained intact for less than two days.² For this reason, we routinely employ a Gum Mastic Liquid Adhesive which serves as a non-water soluble tackifier for the skin and enables a high probability for the dressing to remain intact for seven days. The Gum Mastic adhesive is particularly helpful in patients with clammy or diaphoretic skin.
The Solution
Vascular Access is the most prevalent invasive medical procedure and can have serious, even fatal consequences. The Insertion Bundle is standardized around the world and has been credited with drastically reducing Blood Stream Infections. However, the Insertion Bundle takes ten minutes to perform and there is a lot more to successful Vascular Access than the Insertion Bundle. The C&M by the nursing staff is the dominant phase of the Life Cycle. The C&M depends on a proper, standardized Insertion which includes a dressing that remains intact for seven days. Gum Mastic Liquid Adhesive is an inexpensive solution to dressing disruption.